62 yr old male patient with shortness of breath and pedal edema
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:
A 62 yr old male patient, a toddy tree climber, came with c/o shortness of breath, b/l pedal edema and giddiness since 6 days.



Patient was apparently asymptomatic 6 days back and then he developed shortness of breath since 6 days
Sudden onset , associated with food intake
No h/o chest pain , cough , palpitations , orthopnea , PND , sweating.
Pedal edema since 6 days
B/l pitting type , painless , gradually increasing on prolonged sitting
No h/o decreased / increased urine output ,burning micturition , fever, pain abdomen, abdominal distention.
Giddiness 4-5 episodes , each lasting for 15 - 20 mins.
No postural variation / headache / LOC / blurring of vision / nausea / vomiting / tinnitus.
Past history
Not a k/c/o DM , HTN , Asthma , epilepsy , CAD , TB , CVA , Thyroid
Personal history:-
Diet - mixed
Bowel - regular
Bladder - regular
Chronic alcoholic
Toddy 90ml daily since 40 yrs
Whisky 60ml / Beer 750ml every 10-15 days for 20 yrs
Smoker 1-2 beedis every day for 40yrs, stopped 6 months ago
On examination:-
Pt consicous, coherent, cooperative
Thin built
Pedal odema +
No pallor, icterus, clubbing, cyanosis, lymphadenopathy.
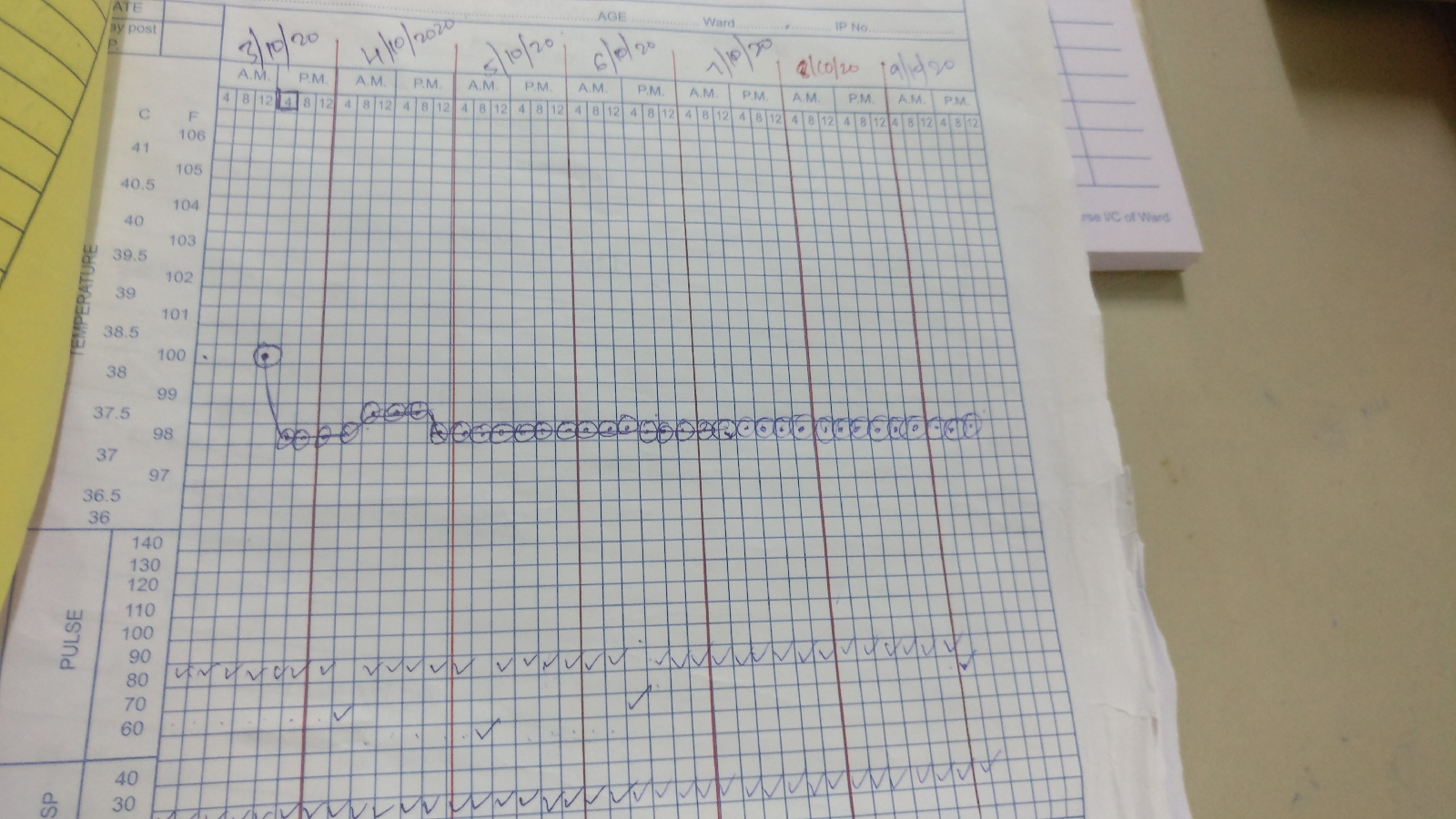
Temp : 98.4 F
PR : 97 bpm , irregularly irregular
BP : 120/70 mmhg



CVS :
Inspection- Apex beat visible in 6th ICS 1cm lateral to MCL.
Visible scars in precordium area.
Carotid pulsations seen
No engorged veins or visible sinuses
Raised JVP, upto angle of mandible
Palpation- Inspectory findings are confirmed
Apex impulse felt in 6th ICS 1cm lateral to MCL
No pulsations, palpable sounds or thrills felt in mitral, tricuspid, aortic and pulmonary areas.
Auscultation- S1 S2 +
High pitched , Grade 3 , Pan systolic murmer is present in all 4 areas , best heard in mitral area with diaphragm and radiating to axilla
RS :
Inspection-
Upper respiratory tract- Normal
Shape of chest- Pectus excavatum
Symmetry of chest- left nipple lower than right
Trachea- central
Back - scoliosis to the right, deformity ( swelling) over right scapular and infrascapular area ( common in toddy tree climbers)
Palpation- Inspectory findings confirmed
Chest wall symmetry- Shape- elliptical
AP diameter- 15cm
Transverse diameter- 26cm
Hemithorax Size- right is 42cm, left is 38cm
Total expansion- 3cm
Vocal fremitus- decreased in rt infrascapular and increased in rt suprascapular
Percussion- Dull note in right infrascapular and infra axillary areas
Auscultation- BAE + , Decreased air entry in right infrascapular area
Crepts + in right and left infrascapular areas and right infra axillary area
P/A : soft , non tender , Hepatomegaly + (liver span : 15cms), hypopigmented spots in epigastrium ( sensations +)
Investigations
Day 1










DAY 2



TREATMENT
Day 1
TAB.LASIX 20mg PO BD 2-----0------1
Fluid restriction <1.5 lit/day
Strict I/O monitoring
Day 2
Tab Lasix 20 mg PO BD 2----0-----1
Tab Telma 20mg PO OD
Fluid restriction <1.5 lit/day
Day 3
Tab Lasix 20 mg PO OD
Tab Telma 20mg OD
Tab Ecosprin 75mg PO OD
Tab Clopidogrel 75mg PO OD
Tab Atoruastatin 20 mg PO OD
Fluid restriction <1.5 lit/day
Patient is being referred to higher centre for CT coronary angiogram